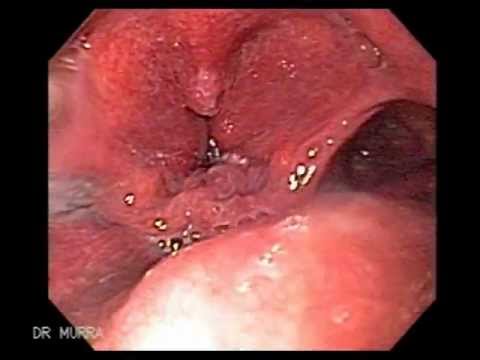
Larynx Cancer with Orotracheal invasion
Laryngeal cancer is the most common cancer of the upper aerodigestive tract. The incidence of laryngeal tumors is closely correlated with smoking, as head and neck tumors occur 6 times more often among cigarette smokers than among nonsmokers. The age-standardized risk of mortality from laryngeal cancer appears to have a linear relationship with increasing cigarette consumption. Death from laryngeal cancer is 20 times more likely for the heaviest smokers than for nonsmokers.
Furthermore, active smoking by patients with head and neck cancer is associated with significant increases in the annual rate of second primary tumor development compared to former smokers or nonsmokers. The use of unfiltered cigarettes or dark, air-cured tobacco is associated with further increases in risk.
Although alcohol is a less potent carcinogen than tobacco, alcohol consumption is a risk factor for laryngeal tumors. In individuals who use both tobacco and alcohol, these risk factors appear to be synergistic, and they result in a multiplicative increase in the risk of developing laryngeal cancer.
Treatment of laryngeal carcinoma has changed during the last years. At the beginning of the last century, therapies were surgically directed. Total and partial laryngectomy surgeries were and still are the mainstream surgical procedures to treat malignant tumors of the larynx. A paradigm change in treatment was experienced in the early 1990s. The organ preservation treatments using concurrent chemoradiation therapy were introduced. This treatment approach demonstrated survival rates similar to total laryngectomy plus radiation therapy, while preserving the larynx in 63% of the patients. In addition, new developments in endoscopic surgical techniques and laser equipment are opening a new era in the treatment of malignant tumor of the larynx.
Signs or symptoms of larynx cancer are somewhat dependent on where the cancer is growing (supraglottis, glottis, subglottis). Patients with glottic cancer, or cancer that grows on the true vocal cords, often present with the early sign of hoarseness. This occurs because even a slight interference with the vibrating function of the vocal cords can produce voice changes. Hence, any long-standing hoarseness or voice changes should prompt a laryngeal examination. If hoarseness is ignored or if advanced disease occurs, airway obstruction, pain, or difficulty swallowing can result.
Supraglottic cancers usually do not produce early signs or symptoms, so supraglottic cancers are more often in advanced stage upon diagnosis. Hoarseness can also occur with supraglottic cancer, though usually later in the disease state. Also, in patients with supraglottic cancer, voice changes referred to as “hot potato voice” can occur. This can be described as the type of voice someone would speak in if they had a piece of hot food (potato) in their mouth. In addition to voice changes, patients can also present with pain, problems swallowing, or even ear pain, which can result from the involvement of nerves in the throat by the tumor. Supraglottic cancers often spread to lymph nodes in the neck, and many patients notice a lump in the neck as the first sign of cancer. Any lump or bump in the neck that does not go away within a few days should be evaluated by a physician.
Subglottic cancers are fairly rare, though they also fail to produce early symptoms. Therefore, they also present in more advanced stages and patients can have signs of disease similar to that of supraglottic cancers.
Again, these signs and symptoms are nonspecific and could represent a variety of different conditions-both benign and malignant. However, if you have any of these symptoms, especially if they are longstanding or if you are a smoker, you should see your physician.